High-quality CPR is vital to ensure a victim of cardiac arrest has the best possible chance of survival. CPR is a practical skill, and surprisingly easy to make mistakes when performing. You should avoid performing these common CPR mistakes:
Inadequate chest compression depth
Chest compressions need to be at least 5cm (2inches) deep in order to be effective. A common mistake made during CPR is performing shallow, ineffective chest compressions. Often people underestimate the force required in order to compress an adult victim’s chest. In addition, some people are worried about causing harm to the victim (for example, rib fractures).
Shallow chest compressions will not provide enough force to pump blood around the victim’s body. Therefore the brain will be starved of vital oxygen and a defibrillator is less likely to work when it is deployed.
It is common for ribs to be broken during CPR. One study found the prevalence of rib fractures in adult victims who received CPR was over 80. The rescuer may feel ribs break when they deliver chest compressions. This can be an unpleasant experience for the rescuer, but it is important to continue to deliver high-quality chest compressions.
Too slow or too fast chest compressions
Chest compressions should be given at a speed of around 100 – 120 a minute. Slow chest compressions are less likely to be effective, and fast chest compressions may not be deep enough in order to push blood around the body.
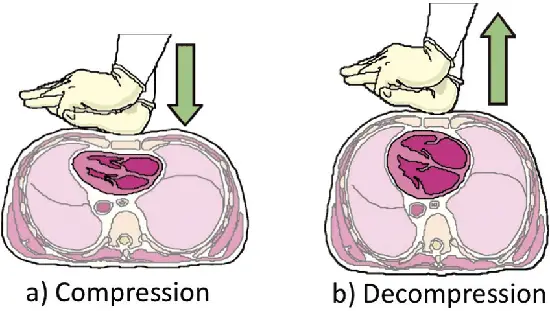
Leaning on the victim’s chest
Each chest compression should involve compressing the chest to a minimum of 5cm, followed by a full release of the chest wall. This is important to allow the heart to fill with blood. A common mistake new rescuers make is to ‘lean’ on the victim’s chest, especially when they become tired. This means there is not a complete release of the chest wall after each compression, reducing the effectiveness of the CPR.
Over-inflating the victim’s lungs
If trained and willing, rescue breaths can be performed in order to provide oxygen to a victim. However, it is important not to over-inflate the victim’s lungs. Over inflating the lungs will cause air to enter the stomach and increase the risk of the victim vomiting and blocking their airway. Therefore, each rescue breath should only last approximately one second.
John Furst
JOHN FURST is an experienced emergency medical technician and qualified first aid & CPR instructor. John is passionate about first aid and believes everyone should have the skills and confidence to take action in an emergency situation.
The actual effective depth is 1/3 rd the front back distance the inches thing is a compromise and we taught that almost 30 years ago
in many cases you don’t break ribs you separate the cartlige that joins the ribs to the sternum
hands only cpr with a head tilt eg a patent airway is the best way for adult cpr passive inspiration of air containing 20 %
not about 16% as in expired air for mouth to mouth
also NEVER use the term look for rise and fall of chest that was when a male weighed 75 kg
talk about a slow gentle inflow of air
the correct calculation for ventilations/ breaths is an estimation of 10 mls of air per body kilo for example a 100 kg person gets 1000 ml
a 50 kg person gets about 500 ml of air or oxygen a child weighing 10 kg get only 100 ml of breath or bag mask
this in itself clarifies that the in trained person is best to stay away from ventilations as they think more is better
resulting in gastric distention / regurgitation and diaphragm splinting
Most of the world except good old Australia the ARC still persists in 30 compressions to 2 ventilations
If they really want to improve things go back to instructing a better course that entails
Respiratory arrest versus cardiac arrest
They also need to stop calling the lateral position the RECOVERY position
In addition they need to stop teaching the stupid chest thrusts for choking
how dumb place someone on their back and push over their heart with gravity against you
the chest thrust is just clinically ridiculous it may be ok for a child on an adult
there used to be a technique called the lateral chest thrust that worked exceptionally well
how do I know I used it quite a few times
Of course I am more that familiar with the other resuscitation physiologies
drowning versus cardiac arrest
the other dumb stupid thing is the blanket statement for crush injury syndrome by the ARC
sure if it less than half a limb or it is on their chest GET IT OFF
picture this a 300 tonne coal truck has drove its wheels over a person legs up to their thighs
the legs are now mush and as soon as you move the truck their will be two affects
yes the ho hum crush syndrome we all talk about
BUT worse is the reperfusion affect as the truck drives off his limbs he dies from hypovolaemia as well as crush syndrome
but I don’t know much I was only a Ambulance Officer / Paramedic /Military Medic 30 years combined



Very important information, I like your first aid tips.
The actual effective depth is 1/3 rd the front back distance the inches thing is a compromise and we taught that almost 30 years ago
in many cases you don’t break ribs you separate the cartlige that joins the ribs to the sternum
hands only cpr with a head tilt eg a patent airway is the best way for adult cpr passive inspiration of air containing 20 %
not about 16% as in expired air for mouth to mouth
also NEVER use the term look for rise and fall of chest that was when a male weighed 75 kg
talk about a slow gentle inflow of air
the correct calculation for ventilations/ breaths is an estimation of 10 mls of air per body kilo for example a 100 kg person gets 1000 ml
a 50 kg person gets about 500 ml of air or oxygen a child weighing 10 kg get only 100 ml of breath or bag mask
this in itself clarifies that the in trained person is best to stay away from ventilations as they think more is better
resulting in gastric distention / regurgitation and diaphragm splinting
Most of the world except good old Australia the ARC still persists in 30 compressions to 2 ventilations
If they really want to improve things go back to instructing a better course that entails
Respiratory arrest versus cardiac arrest
They also need to stop calling the lateral position the RECOVERY position
In addition they need to stop teaching the stupid chest thrusts for choking
how dumb place someone on their back and push over their heart with gravity against you
the chest thrust is just clinically ridiculous it may be ok for a child on an adult
there used to be a technique called the lateral chest thrust that worked exceptionally well
how do I know I used it quite a few times
Of course I am more that familiar with the other resuscitation physiologies
drowning versus cardiac arrest
the other dumb stupid thing is the blanket statement for crush injury syndrome by the ARC
sure if it less than half a limb or it is on their chest GET IT OFF
picture this a 300 tonne coal truck has drove its wheels over a person legs up to their thighs
the legs are now mush and as soon as you move the truck their will be two affects
yes the ho hum crush syndrome we all talk about
BUT worse is the reperfusion affect as the truck drives off his limbs he dies from hypovolaemia as well as crush syndrome
but I don’t know much I was only a Ambulance Officer / Paramedic /Military Medic 30 years combined
I like your first aid tips